
Cardiac Surgeon Pioneers Minimally Invasive Aortic Valve Procedure
Architect Andres Duany was undergoing a full clinical assessment when he received the unsettling news. He needed heart surgery to replace a bicuspid aortic valve, a genetic abnormality.
“I knew I had it, but I showed no symptoms,” he recalls. “I was so caffeinated all the time — 8 to 10 espressos a day — that maybe I didn’t notice.”
Duany, a star architect who is known, along with his wife, for hundreds of projects under the New Urbanism movement, proceeded to research his options. He preferred minimally invasive surgery — “I didn’t want a big scar” — and he wanted the best surgeon to perform the delicate operation.
I did lots of research and made lots of inquiries with friends. I always ended up with the same name — Lamelas.
Andres Duany

At the time, Dr. Joseph Lamelas, a world-renowned cardiac surgeon for his pioneering of minimally invasive techniques, worked at Baylor College of Medicine in Houston. The distance didn’t deter Duany, however, and now, about 14 months later, he’s eager to sing his surgeon’s praises. During the procedure, Dr. Lamelas not only replaced his valve but also the entire ascending aorta.
“He responded with commendable ability,” Duany notes.
Duany was out of the hospital in three days and in pain for only 10 days — a sharp contrast to the more invasive traditional surgery that involves the breaking of the breastbone. By three weeks he was back to his regimen of push-ups. “I can’t even find my scar,” he jokes. “It’s somewhere under my armpit.”
The “Miami Method”
A self-declared “huge fan” of Dr. Lamelas, Duany is delighted that the surgeon has returned to Miami, where he now heads the Department of Cardiothoracic Surgery at the University of Miami Health System. His arrival is sure to attract patients from around the world, as he’s internationally known for a series of minimally invasive cardiac surgery techniques known as the “Miami Method.” He is also the only surgeon who uses a minimally invasive method to replace an ascending aorta through a small incision between the ribs, the procedure Duany underwent in Texas.
Dr. Lamelas only began using his ascending aortic technique in 2012, after years of working with minimally invasive methods for other cardiac surgeries, including the repair and replacement of the mitral valve, aortic valve, double and triple valves, as well as tumor removal and congenital cardiac defects. The traditional method for aorta repair requires opening up the chest and splitting the entire sternum to get to the heart. This allows the surgeon more visibility — but it also means more pain, more bleeding and a longer recovery time for the patient. Though minimally invasive methods result in similar outcomes with less trauma, not every doctor is willing, or capable enough, to work through a much smaller incision, in a restricted space, and with difficult-to-master instruments.
But Dr. Lamelas plans to continue developing this very specialized minimally invasive technique. “My goal is to perfect this and to make it available to all my patients.”
The anatomy of an aorta
To understand the complexity and difficulty of the surgery, a brief lesson in the anatomy of the aorta, the body’s largest artery, is required.
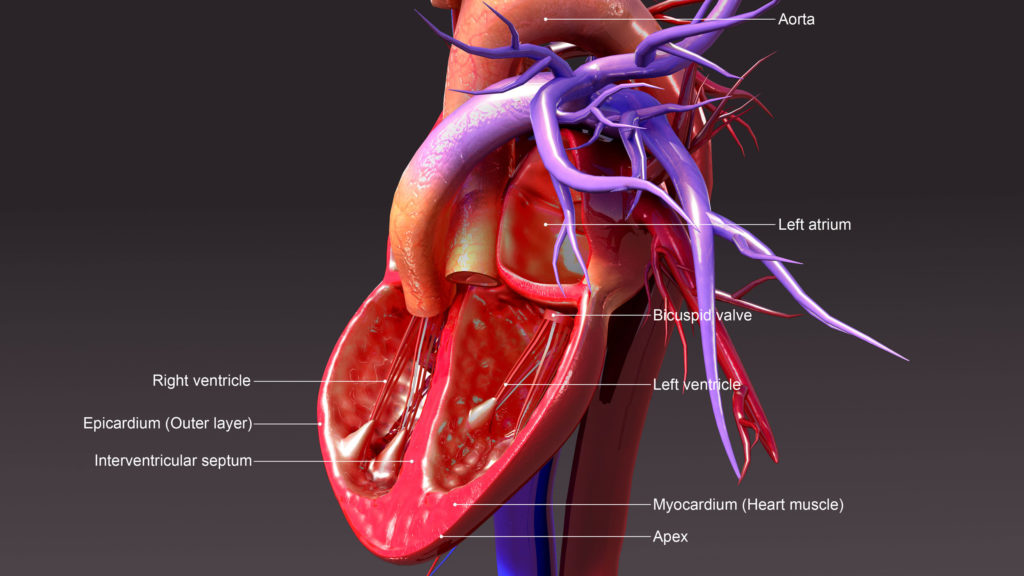
Imagine the ascending aorta as the top of a twisting candy cane that goes up, forward and to the left. It’s about 4 to 5 inches long and a little more than 2 inches in diameter. It begins from the left ventricle, where the heart pumps blood out through the aortic valve into the curving part of aorta. The aortic valve has three doors that open and close with each heartbeat to allow the blood to flow out and not return into the heart. Two coronary arteries, which provide blood to the heart muscle, branch out from right above the aortic valve.
Duany’s biscuspid valve — a condition in which the valve has two doors instead of three —occurs in 1 to 2 percent of the population. But this defect can be dangerous as it often results in aortic insufficiency, where the blood flows back into the heart, or stenosis, a narrowing or blockage of the aortic valve which forces the heart to work harder.
Because of the ascending aorta’s location and size, replacing the aorta through a small incision on the right side of the chest is a “much more challenging” procedure. Lamelas explains. “You need a lot of experience and practice to get comfortable [with minimally invasive techniques.] It’s a longer learning curve. You just don’t jump into the saddle and start these complex cases from day one. ”
Several aortic conditions require surgery
One of the more common is an aortic aneurysm, which occurs when the blood vessel bulges out, stretching the aortic walls like an over-filled balloon. Though aneurysms tend to be slow-growing, physicians must watch them closely because an aneurysm can eventually lead to a rupture of the blood vessel. When an aneurysm grows from 4.5 to 5.5 cm, surgery is indicated.
Aneurysms, Dr. Lamelas explains, can be an isolated condition but many are also accompanied by some kind of aortic valve defect, including a narrowing or a leak of the valve. In such cases of valve stenosis or valve regurgitation, he can repair both using his specialized technique. (If the aneurysm appears in the aortic arch, however, it is not possible to use minimally invasive techniques.)
Another condition that requires surgery is aortic dissection, when the aorta wall tears. This condition can be life-threatening and surgery is required as soon as it’s diagnosed.
Dr. Lamelas begins by making an incision of about 5 cm (or two inches) between the ribs on the right side. Then, depending on what the patient needs, he begins replacing either the ascending aorta itself or the aortic valve — or both. He completely cuts out the diseased area of the aorta and replaces it with synthetic fabric such as a Dacron graft. He then replaces the valve depending upon its condition. A valve can be repaired by several different techniques or replaced with a mechanical valve or one made from pig or cow tissue.
No room for error
Because of Dr. Lamelas’ extensive experience, he tailors the operation to the patient’s needs. He has developed a multitude of techniques to perform this delicate operation which has no room for error. He has even replaced the entire ascending aorta and hemi arch along with replacing the aortic root. This entails detaching the coronary arteries from the base of the aorta along with the aortic valve. Thereafter, he replaces the aortic valve and reimplants the coronaries into the Dacron graft, which substitutes for the ascending aorta. This is known as a Bentall Procedure.
A typical ascending aortic surgery lasts about four hours, about half the time of an open procedure, and results in both a shorter hospital stay and faster recovery time. This is especially encouraging for elderly patients, many of whom are denied traditional aortic surgery based on age and high-risk health profiles.
“There is no best candidate profile,” explains Dr. Lamelas, who performs an average of 5 of these ascending aortic procedures a month. “It can be offered to anyone.”
For patients like Duany, Dr. Lamelas’ groundbreaking techniques are, as the architect describes them, “nothing short of a miracle.” At 69, the architect feels like he’s been given a new lease on life.
“I feel superb,” Duany says. “It’s like I’m Superman. People come to me out of the blue and say, ‘You look so good!’”
Ana Veciana-Suarez, Guest Columnist
Ana is a regular contributor to the University of Miami Health System. She is a renowned journalist and author, who has worked at The Miami Herald, The Miami News, and The Palm Beach Post. Visit her website at anavecianasuarez.com or follow @AnaVeciana on Twitter.
Tags: ascending aorta, Bentall Procedure, cardiac surgery, cardiothoracic surgery, Dr. Joseph Lamelas
{kind=link}
{kind=link}